
Migraines: Are They More Than a Headache?

Sometimes migraines can be a real headache. But they’re rarely only a headache. Headaches are perhaps the most common symptom of a migraine, but they are only part of a sequential, cyclical process for many people. Migraines are exceptionally common, affecting an estimated one billion people worldwide, which means one in every eight people suffers from them! This makes them the second leading cause of disability worldwide after low back pain. Women are more likely to get migraines. Most people with chronic migraines start getting them in childhood, and they progress through adulthood. Migraines fall into two major categories. Episodic migraine is when a person has fewer than 15 days a month experiencing migraines, and chronic migraine is 15 or more days a month for at least 3 months.
Migraines are a complex brain disorder. They have five main phases, though not every patient experiences each of these phases, and it may also vary from attack to attack.
- The prodrome phase consists of warning signs that signal an oncoming migraine.
- Aura is a phase immediately before the attack which may have temporary neurological symptoms, including sensitivity to light and sound.
- Headache is the most typical symptom during a migraine attack and is frequently accompanied by nausea, vomiting, sensory changes, and gastrointestinal symptoms.
- Postdrome is like a hangover, with lingering symptoms without a headache.
- Finally, the interictal phase is the period between migraines that often lasts for days or years.
Patients report that sleep, relaxation, food, and darkness may help move from an attack to the postdrome or interictal phase. Though people frequently think of a migraine as just the headache from a migraine attack, it really starts with prodrome. Let’s pick our brains about the prodrome phase.
Around ⅓ of migraine sufferers experience prodrome. It can last anywhere from minutes to over 12 hours, though around 2 hours seems typical. The most common symptom seems to be gastrointestinal problems like diarrhea and constipation. Other common symptoms include mood changes, stiffness in the neck, tiredness, and yawning. Food cravings and abnormal sensitivity to light and sound often occur. Prodrome progresses to a full migraine attack around 70% of the time, though this varies wildly between individuals. Let’s think about what might be going on inside (and outside!) of our skulls.
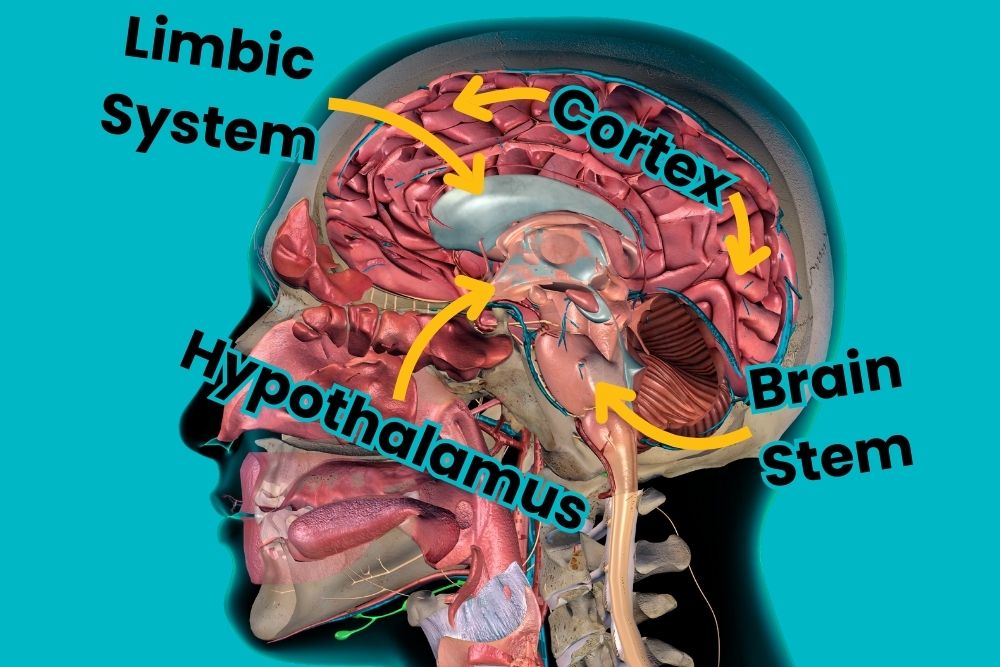
We can look at symptoms to guess what might be happening inside. Changes in mood may point to the limbic system, a collection of brain structures responsible for emotion and behavior. Abnormal sensations indicate cortical differences, particularly in the visual and sound centers of the brain - or the pathways leading to them. Muscle tenderness or stiffness of the neck suggests the brainstem is involved. Many of the other symptoms include fatigue, yawning, depression, irritability, food cravings, nausea, and GI problems, which give a strong indication that the hypothalamus is involved. The hypothalamus is an evolutionarily ancient part of the brain and acts as a crossroads of different information. Sensory information goes to the hypothalamus before being passed on, and it also talks to the endocrine system (responsible for hormones), the involuntary nervous system, sleep/wake cycles, and behavior systems. It tries to maintain stability throughout the brain and body, a process called homeostasis. Nearly every migraine patient reports at least one hypothalamus-mediated symptom.
The brain areas involved give a good indication of what may be happening during the prodrome phase. Sensitivity to light, sound, stress, and hormones seems to increase during prodrome. The hypothalamus fails to maintain homeostasis. Indeed, patients with prodromes report more triggers, more diverse triggers (like alcohol, perfumes, stress), longer aura and attack phases, and a higher chance of postdrome. How these prodrome symptoms change to the later phases of migraine is difficult to see, but we have a few theories. To understand how these may relate to the painful headaches typical of migraines we have to look at how the brain feels pain.
Pain is reported to the brain through pain receptors, also called nociceptors. Nociceptors are found throughout the body, but are notably absent from the brain. Painful headaches during migraines are thought to be from the brain reading pain signals from the area outside of our skull - on the top of our head, in the neck, and so on. These pain signals travel to the brain through, you guessed it, the hypothalamus. It is unclear how prodrome changes to the hypothalamus might set the stage for painful migraine attacks. The hypothalamus may overreact to changes in homeostasis, causing activation of nociceptors, changes to blood vessel size, and the release of neurotransmitters that disrupt the brain and make it susceptible to attack. The hypothalamus may also work with the brainstem to lower the threshold for painful stimuli from nociceptors on the head to get through and cause your head to hurt. The cells that transport pain information become more sensitive, meaning lower amounts of pain elicit a bigger feeling in the brain.
Looking at the hypothalamus during prodrome symptoms also gives a good clue on how people find relief from migraines. Restoring homeostasis in the brain may help reset the hypothalamus and other related systems. Methods to restore homeostasis undoubtedly vary from person to person, but may include eating, sleeping, relaxing, and lowering external stimulation (with a quiet and dark room, for instance). When this isn’t enough, migraine medications can help. Preventive therapies try to lower the number and severity of migraines in the future and may include blood pressure medications, seizure medications, antidepressants, and even things like botox! Acute migraine medications aim to restore balance and end a headache that’s happening now, but several lose effectiveness if used too frequently. As research into migraines continues, we can put this headache of a condition behind us.
Staff Writer / Editor Benton Lowey-Ball, BS, BFA
Click Below for ENCORE Research Group's Enrolling Studies

References:
Burstein, R., Noseda, R., & Borsook, D. (2015). Migraine: multiple processes, complex pathophysiology. Journal of Neuroscience, 35(17), 6619-6629. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4412887/
Kelman, L. (2004). The premonitory symptoms (prodrome): a tertiary care study of 893 migraineurs. Headache: The Journal of Head and Face Pain, 44(9), 865-872. https://doi.org/10.1111/j.1526-4610.2004.04168.x
Koren, M. J., Toenjes, S. (May 13, 2024). Two docs talk: Migraines. MedEvidence Podcast. (Podcast). https://medevidence.com/two-docs-talk-migraines
International Headache Society. (2019). 1.3 Chronic migraine https://ichd-3.org/1-migraine/1-3-chronic-migraine/ Accessed 15 Jan 2024.
Maniyar, F. H., Sprenger, T., Monteith, T., Schankin, C., & Goadsby, P. J. (2014). Brain activations in the premonitory phase of nitroglycerin-triggered migraine attacks. Brain, 137(1), 232-241. https://academic.oup.com/brain/article/137/1/232/363839
May, A., & Burstein, R. (2019). Hypothalamic regulation of headache and migraine. Cephalalgia, 39(13), 1710-1719. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7164212/
Saper, C. B., & Lowell, B. B. (2014). The hypothalamus. Current Biology, 24(23), R1111-R1116. https://www.sciencedirect.com/science/article/pii/S0960982214012998

